- Messages
- 1,241
- Reactions
- 2,505
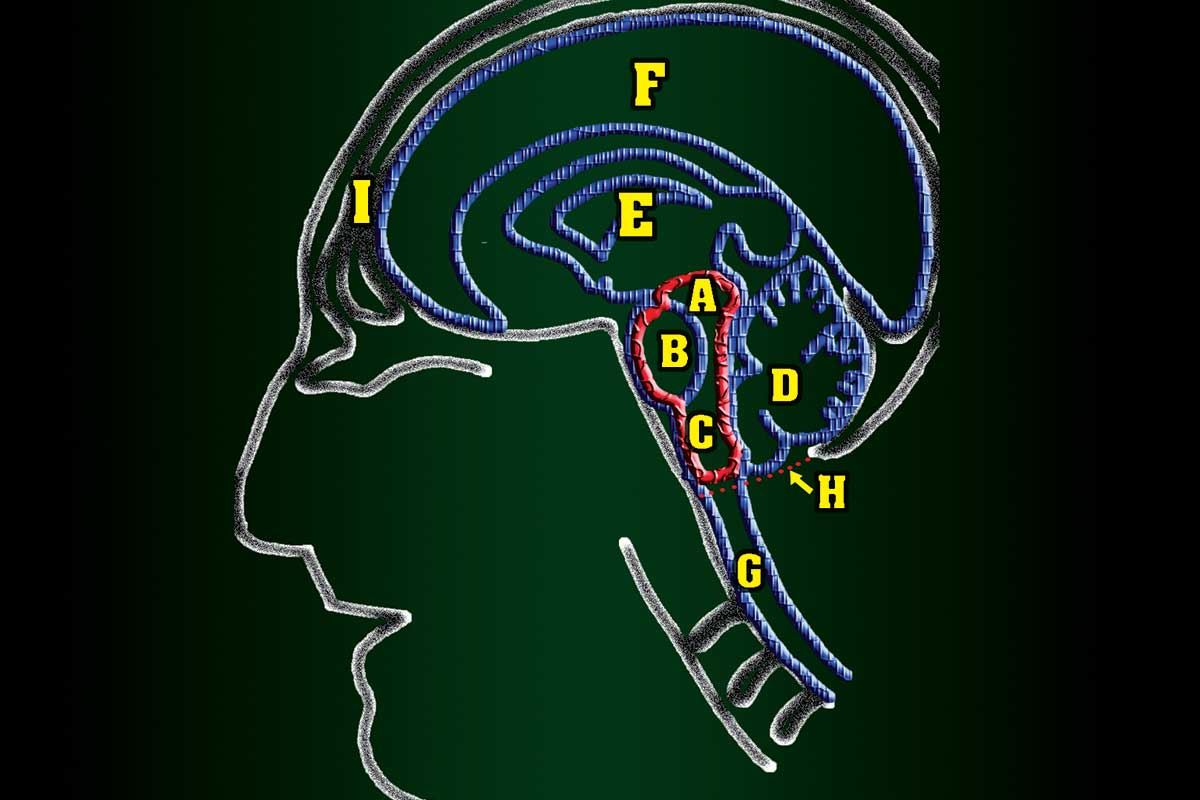
SHOOTING WITH X-RAY VISION PART II | Ethics Of Deadly Force Training - American Cop
At a 2007 law enforcement training conference the wife of one of the attendees criticized me sharply for training cops in Tactical Anatomy. She contended, quite rightly, if cops shoot more effectively more felons are going to be killed. “Excuse me,” I replied. “What part of the term “deadly...
americancop.com
I had never thought of facing bad guys wearing body armor until I read this. Brings a new concern to me if I am faced with a gravest extreme situation.